MedicoNotes @MedicoNotes
Professionally designed high-yield medical notes to help you prepare for exams and excel in clinical practice📝 - visit our website for e-books ⬇️ mediconotes.com Joined September 2015-
Tweets2K
-
Followers7K
-
Following6
-
Likes201
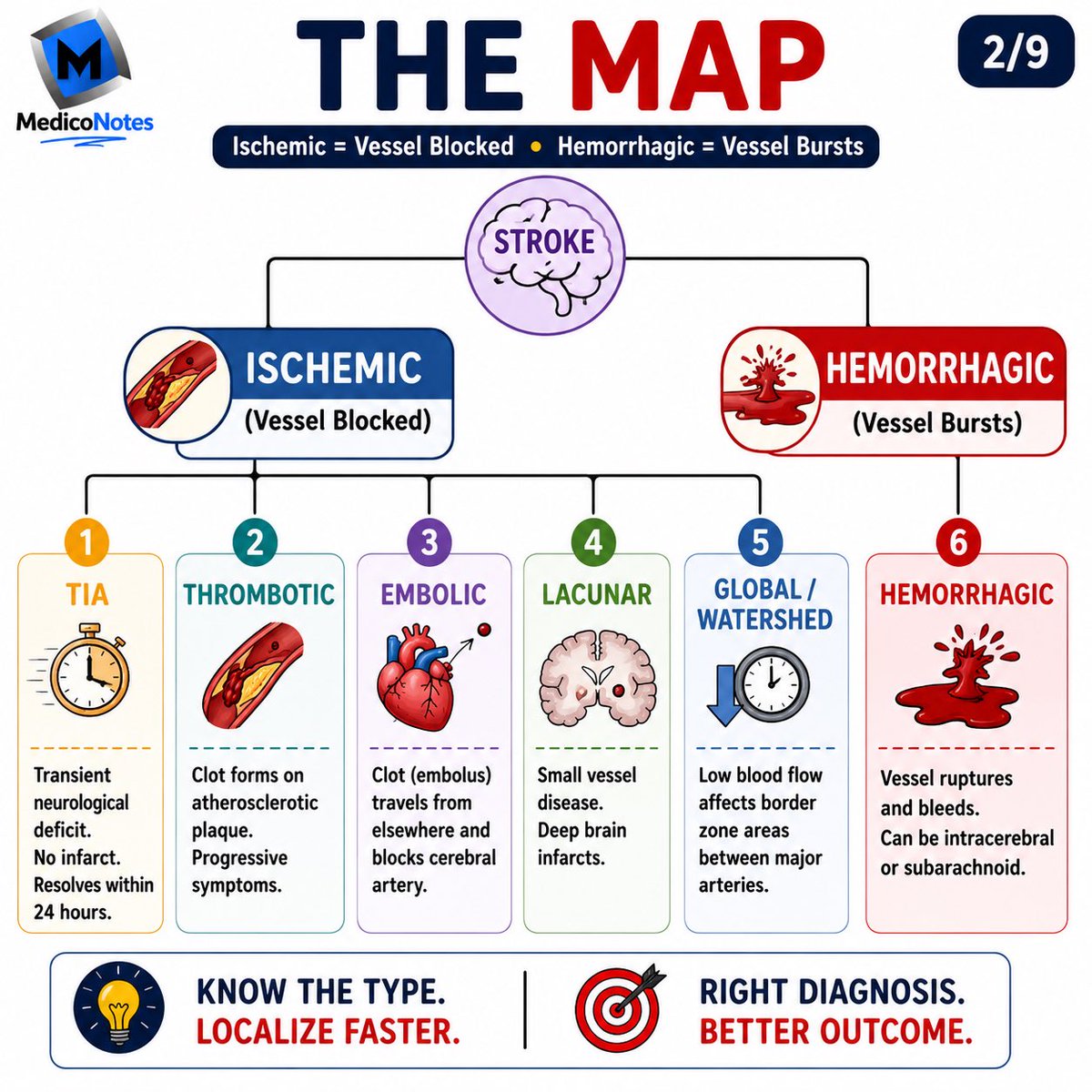
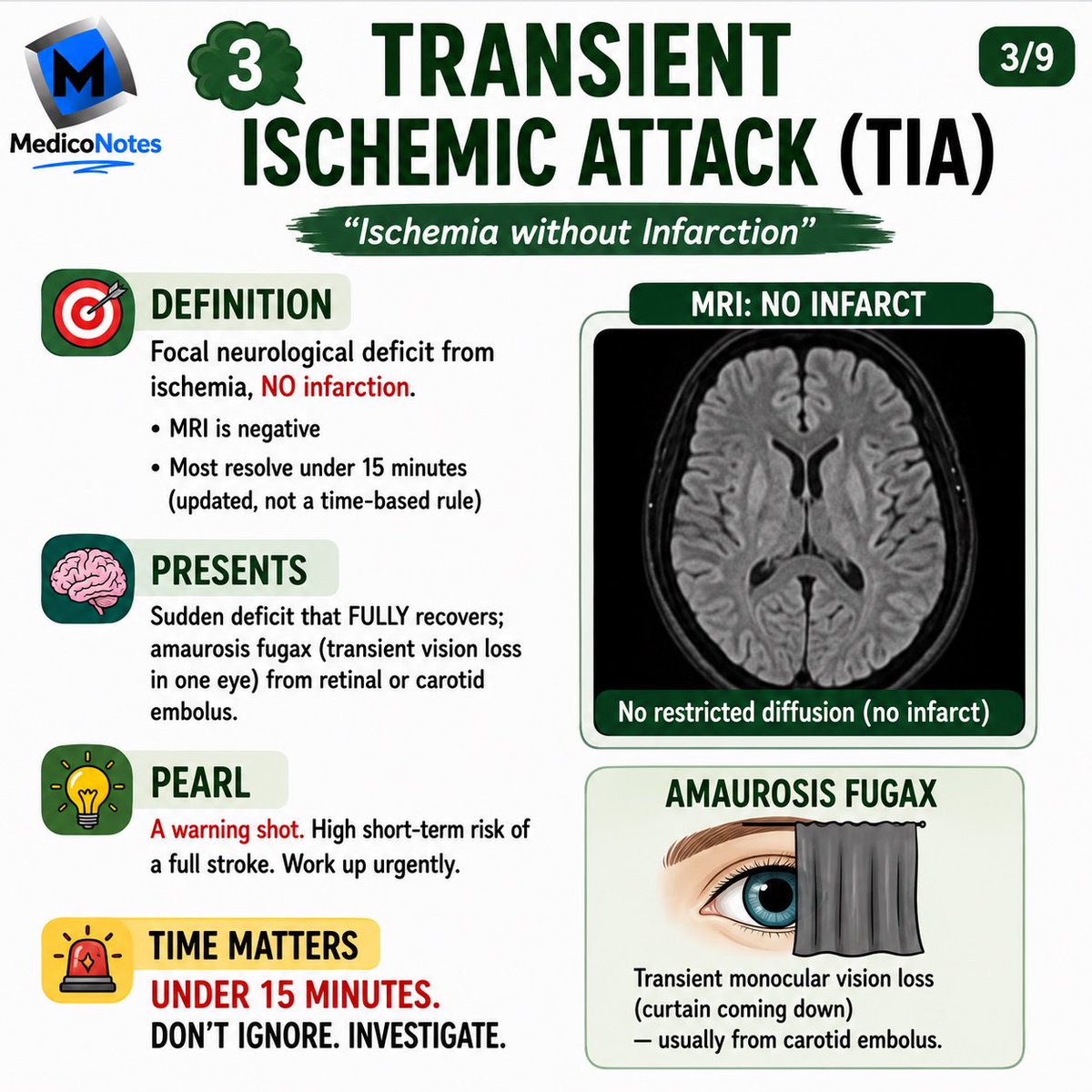
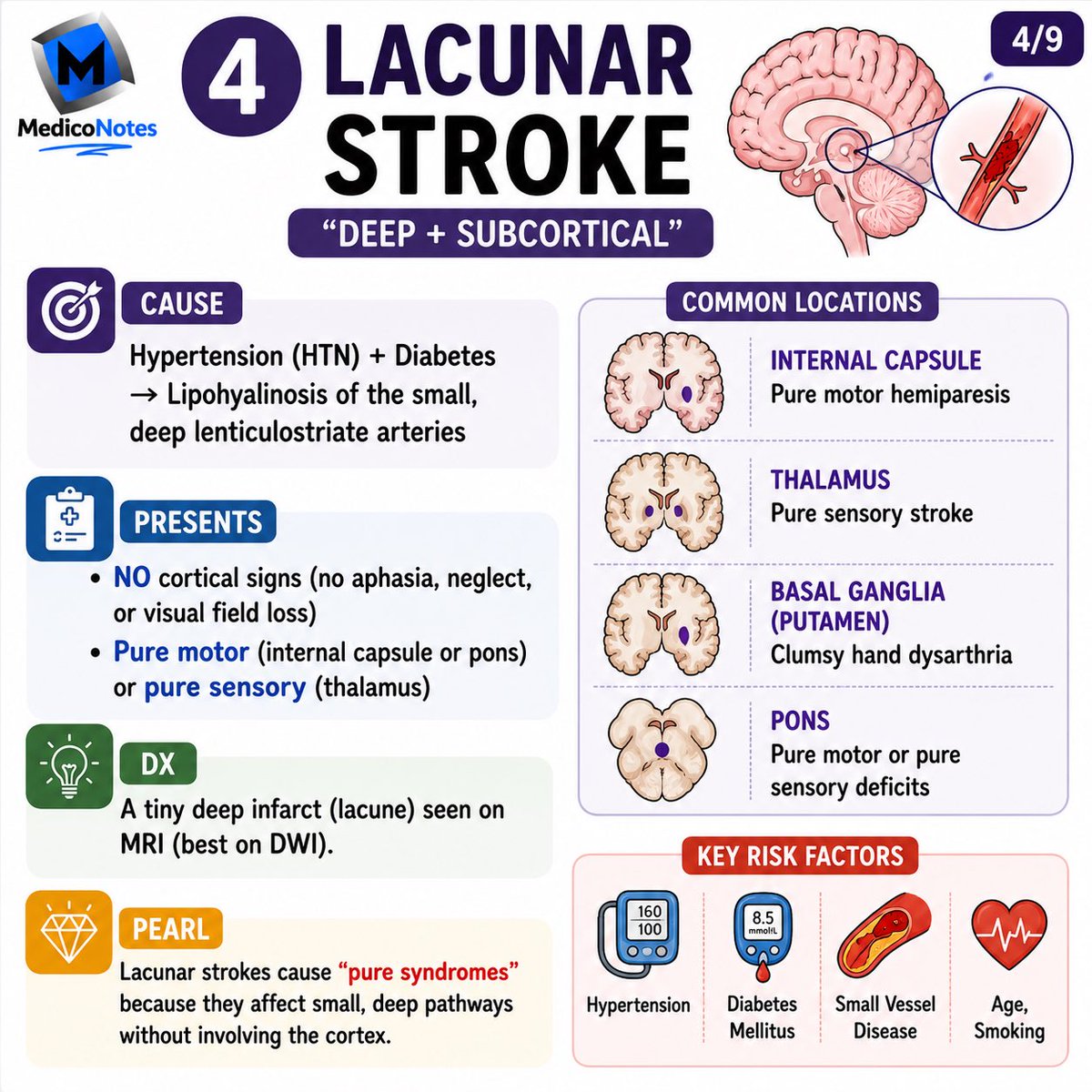
🧠 6 Types of Stroke ⸻ 1️⃣ Types of Stroke ➊ Transient Ischemic Attack (TIA) * Transient focal neurological deficit without cerebral infarction * MRI diffusion-weighted imaging is negative * High short-term risk of subsequent stroke ➋ Thrombotic Stroke * Thrombus forms on an atherosclerotic plaque * Progressive reduction in cerebral blood flow * Often associated with carotid or intracranial atherosclerosis ➌ Embolic Stroke * Embolus travels from the heart or proximal arteries to the brain * Sudden onset neurological deficit * Commonly caused by atrial fibrillation, recent MI, or carotid plaque ➍ Lacunar Stroke * Small vessel occlusion due to chronic hypertension and diabetes * Produces deep subcortical infarcts * Causes classic pure motor or pure sensory syndromes ➎ Watershed (Global Hypoxic) Stroke * Results from severe hypotension or systemic hypoperfusion * Involves border zones between major cerebral arteries * May cause bilateral proximal limb weakness (“man-in-the-barrel” syndrome) ➏ Hemorrhagic Stroke * Due to rupture of an intracranial vessel * Includes intracerebral hemorrhage and subarachnoid hemorrhage * Associated with raised intracranial pressure and mass effect ⸻ 2️⃣ Clinical Presentation Typical features include: * Sudden unilateral weakness or numbness * Facial droop * Dysarthria or aphasia * Visual loss or visual field defects * Ataxia or vertigo * Altered consciousness (more common in hemorrhagic stroke) 💡 Remember FAST: Face drooping • Arm weakness • Speech difficulty • Time to seek emergency medical care. ⸻ 3️⃣ Diagnosis ➊ Non-contrast CT head is the first investigation to distinguish ischemic from hemorrhagic stroke. ➋ MRI with diffusion-weighted imaging is the most sensitive test for acute ischemia. ➌ Additional investigations: * CT angiography or MR angiography * ECG (look for atrial fibrillation) * Echocardiography * Carotid Doppler/vascular imaging * Blood glucose, coagulation profile, lipid profile ⸻ 📖 Get our high-yield Neurology book now: 🌐 mediconotes.com #Neurology #Stroke #MedicalEducation #MRCP #mediconotes

🧠 MCA vs ACA vs PCA — Localise the Stroke in 5 seconds! ⸻ 1️⃣ MCA — Middle Cerebral Artery 🔸 Contralateral Face & Arm weakness 🔸 Contralateral Face & Arm sensory loss 🔸 Aphasia → if dominant hemisphere 🔸 Gaze deviation TOWARD the lesion 🔸 Visual field: Contralateral Homonymous Hemianopia 🧩 Why? MCA supplies the lateral cortex — face, arm, and language areas ⸻ 2️⃣ ACA — Anterior Cerebral Artery 🔸 Contralateral LEG weakness (arm spared!) 🔸 Contralateral LEG sensory loss 🔸 Abulia / Apathy → behavioural changes 🔸 Urinary incontinence 🔸 Visual field: Contralateral Homonymous Hemianopia 🧩 Why? ACA supplies the medial frontal and parietal lobes — leg area and motivation circuits ⸻ 3️⃣ PCA — Posterior Cerebral Artery 🔸 Contralateral Visual Field Loss → often isolated 🔸 Visual Hallucinations → Charles Bonnet Syndrome 🔸 Visual Agnosia → impaired visual recognition 🔸 Visual field: Contralateral Homonymous Hemianopia with macular sparing 🧩 Why? PCA supplies the occipital lobe (vision) and inferior temporal lobe (visual memory) ⸻ 🧩 The 5-Second Localisation Rule ➊ Face + Arm weak + Aphasia → MCA ➋ Leg weak + Behavioural change → ACA ➌ Vision loss only + Hallucinations → PCA ⸻ ⚠️ The Exam Trap 🔹 All three can cause Contralateral Homonymous Hemianopia 🔹 ACA and MCA → full field defect 🔹 PCA → macular SPARING (occipital cortex has dual blood supply) ⸻ 📚 Master all neurology conditions in our high-yield neurology book: 🔗 mediconotes.com ⸻ #StrokeSyndromes #Neurology #medicine #internalmedicine #usmle

🧠 7 Cranial Nerve Palsies You Must Recognize 1️⃣ CN III – Oculomotor • Ptosis, dilated pupil, and a “down & out” eye. • Think posterior communicating artery aneurysm until proven otherwise. 2️⃣ CN IV – Trochlear • Vertical diplopia, worse looking down or walking downstairs. • Patients often tilt their head away from the affected side. 3️⃣ CN VI – Abducens • Failure to abduct the eye → horizontal diplopia. • May be the first sign of raised intracranial pressure. 4️⃣ CN VII – Facial • Ipsilateral facial weakness with inability to close the eye. • Forehead involvement = LMN lesion (Bell’s palsy). • Forehead sparing = UMN lesion (stroke). 5️⃣ CN V – Trigeminal • Facial sensory loss and weakness of mastication. • Classic cause of trigeminal neuralgia with severe facial pain. 6️⃣ CN VIII – Vestibulocochlear • Hearing loss, tinnitus, and vertigo. • Think vestibular schwannoma in progressive unilateral symptoms. 7️⃣ CN XII – Hypoglossal • Tongue deviates towards the side of the lesion. • Associated with dysarthria and ipsilateral tongue wasting. 💡 High-Yield Exam Pearls ✔️ Down & out eye + ptosis + dilated pupil = CN III palsy. ✔️ Vertical diplopia + head tilt = CN IV palsy. ✔️ Can’t abduct the eye = CN VI palsy. ✔️ Forehead spared? Think stroke. Forehead involved? Think Bell’s palsy. ✔️ Tongue points towards the lesion in CN XII palsy. 🚨 Clinical Approach ✅ Determine whether the lesion is central (UMN) or peripheral (LMN). ✅ Look for associated brainstem signs or other cranial nerve deficits. ✅ Consider urgent imaging if symptoms are acute, progressive, painful, or associated with altered consciousness. 📖 Want more concise, exam-focused neurology notes? Visit mediconotes.com and explore our Neurology book #Neurology #CranialNerves #Neuroanatomy #MedicalStudent #MedSchool

🦴 RHEUMATOID ARTHRITIS (RA) Rheumatoid arthritis is a chronic autoimmune inflammatory arthritis that primarily affects the small joints of the hands and feet. Early diagnosis and treatment are essential to prevent irreversible joint damage and disability. 🔑 Classic Clinical Features 1️⃣ Symmetrical pain and swelling of the MCP and PIP joints 2️⃣ Morning stiffness lasting more than 60 minutes 3️⃣ Warm, tender, swollen joints 4️⃣ Reduced grip strength 5️⃣ Fatigue, malaise, and weight loss 6️⃣ Progressive joint deformities if untreated (ulnar deviation, swan-neck and boutonnière deformities) 🩺 Examination Findings • Tender, boggy synovitis • Symmetrical joint involvement • Reduced range of motion • Rheumatoid nodules (advanced disease) • Hand deformities in long-standing RA 🔍 Investigations • Rheumatoid factor (RF) • Anti-CCP antibodies (most specific) • ESR and CRP • FBC (anaemia of chronic disease) • X-rays of hands and feet • Musculoskeletal ultrasound or MRI for early synovitis 💉 Management 1️⃣ Refer early to Rheumatology. 2️⃣ Start DMARDs as soon as possible (usually Methotrexate). 3️⃣ Short-course corticosteroids may be used as bridge therapy. 4️⃣ NSAIDs for symptom relief when appropriate. 5️⃣ Biologic therapies (e.g. TNF inhibitors, IL-6 inhibitors, JAK inhibitors) for refractory disease. 6️⃣ Physiotherapy, occupational therapy, regular exercise, and smoking cessation. ⚠️ Complications • Joint destruction and deformity • Tendon rupture • Cervical spine instability • Osteoporosis • Interstitial lung disease • Cardiovascular disease 💡 High-Yield Pearl Symmetrical small-joint arthritis + morning stiffness lasting >1 hour = Think Rheumatoid Arthritis. Early treatment within the “window of opportunity” significantly reduces long-term joint damage and improves quality of life. 📚 Save this post and master Rheumatology with our high-yield Musculoskeletal Notes! 🌐 MedicoNotes.com #RheumatoidArthritis #medicaleducation #medicine #doctorsofinstagram #usmle
💡 ACUTE APPENDICITIS Acute appendicitis is one of the most common surgical emergencies. Prompt diagnosis and early surgical referral reduce the risk of perforation, abscess formation, and sepsis. 🔑 Classic Clinical Features 1️⃣ Periumbilical pain migrating to the right iliac fossa 2️⃣ Loss of appetite (often the earliest symptom) 3️⃣ Nausea and vomiting 4️⃣ Fever and tachycardia 5️⃣ Right iliac fossa tenderness with guarding 6️⃣ Rebound tenderness or percussion tenderness 🩺 Examination Findings • McBurney’s point tenderness • Rovsing’s sign • Psoas sign (retrocaecal appendix) • Obturator sign (pelvic appendix) • Localised peritonism 🔍 Investigations • FBC → Raised white cell count • CRP → Elevated • Urinalysis → Exclude urinary causes • β-hCG → In women of childbearing age • Ultrasound → Children and pregnancy • CT abdomen/pelvis → Most accurate imaging in adults 💉 Management 1️⃣ Keep the patient nil by mouth (NBM) 2️⃣ Start IV fluids and adequate analgesia 3️⃣ Administer IV antibiotics if appendicitis is suspected 4️⃣ Arrange urgent surgical review 5️⃣ Laparoscopic appendicectomy is the standard treatment for uncomplicated appendicitis ⚠️ Complications • Perforation • Appendiceal abscess • Generalised peritonitis • Sepsis 💡 High-Yield Pearl Migratory right iliac fossa pain + anorexia + fever = Think appendicitis until proven otherwise. 📚 Save this post and master Surgery with our high-yield Surgery Notes! 🌐 MedicoNotes.com Our Surgery Book is packed with concise algorithms, emergency presentations, clinical signs, investigations, management pathways. #Appendicitis #GeneralSurgery #EmergencySurgery #AcuteAbdomen #surgery
🧠 7 Causes of Acute Confusion Acute confusion (delirium) is a medical emergency. Always identify and treat the underlying cause—not just the symptom. 📚 7 High-Yield Causes: 1️⃣ Metabolic Disorders • Hypoglycaemia or hyperglycaemia • Hyponatraemia, hypercalcaemia • Uraemia and hepatic encephalopathy 2️⃣ Infections • Meningitis and encephalitis • Sepsis, pneumonia, UTI • Brain abscess 3️⃣ Drugs & Toxins • Sedatives, opioids, anticholinergics • Alcohol intoxication or withdrawal • Recreational drugs and medication toxicity 4️⃣ Cerebrovascular Disease • Ischaemic stroke • Intracerebral haemorrhage • Subarachnoid haemorrhage and subdural haematoma 5️⃣ Trauma • Concussion • Intracranial haemorrhage • Diffuse axonal injury 6️⃣ Systemic Causes • Hypoxia or hypercapnia • Shock or severe hypotension • Cardiac failure and severe anaemia 7️⃣ Neurological Disorders • Post-ictal state after seizures • Brain tumours • Normal pressure hydrocephalus • Non-convulsive status epilepticus 💡 High-Yield Exam Pearls ✔️ Always check blood glucose in every confused patient. ✔️ Fever with altered mental status should raise suspicion for meningitis or encephalitis. ✔️ Sudden confusion with focal neurological deficits is stroke until proven otherwise. ✔️ Review the medication list carefully—drug-induced delirium is common, especially in older adults. ✔️ Remember the 4 Ts of delirium: Toxins, Trauma, Temperature (infection), and Trouble with metabolism. 🚨 Approach to Acute Confusion ✅ Stabilise ABCs and check bedside glucose. ✅ Obtain a focused history, medication review, and neurological examination. ✅ Perform targeted investigations (blood tests, ECG, urinalysis, CT brain ± lumbar puncture when indicated). ✅ Identify and treat the underlying cause promptly. 📖 Want more concise, exam-focused neurology notes? Visit mediconotes.com #Neurology #Delirium #AcuteConfusion #Stroke #EmergencyMedicine

🩺 Approach to Acute Kidney Injury (AKI) AKI is a medical emergency—recognize it early, identify the cause, and intervene before irreversible kidney damage occurs. AKI is defined by a rapid decline in kidney function, resulting in rising serum creatinine and/or reduced urine output. The key to management is determining whether the cause is pre-renal, intrinsic renal, or post-renal. 📚 Stepwise Approach to AKI: 1️⃣ Think AKI • Rising creatinine or oliguria (<0.5 mL/kg/hr). • Review previous renal function and identify high-risk patients. 2️⃣ Confirm the Diagnosis • Repeat renal profile. • Perform urinalysis and monitor urine output. • Review medications, recent contrast exposure, and comorbidities. 3️⃣ Classify the Cause 🟢 Pre-renal: Hypovolemia, sepsis, heart failure, cirrhosis. 🔵 Intrinsic: ATN, glomerulonephritis, AIN, vasculitis. 🟠 Post-renal: Urinary tract obstruction (BPH, stones, malignancy). 4️⃣ Investigate Systematically • Assess volume status and blood pressure. • U&Es, bicarbonate, urinalysis, urine sodium/osmolality. • Renal ultrasound if obstruction is suspected. 5️⃣ Treat the Underlying Cause ✔️ Restore perfusion in pre-renal AKI. ✔️ Stop nephrotoxic drugs (NSAIDs, ACEi/ARB where appropriate). ✔️ Relieve urinary obstruction promptly. ✔️ Correct electrolyte abnormalities and monitor fluid balance closely. 💡 High-Yield Exam Pearls ✔️ ATN is the most common intrinsic cause of AKI. ✔️ Always exclude post-renal obstruction with renal ultrasound. ✔️ Hyperkalaemia, severe metabolic acidosis, pulmonary oedema, and uraemic complications require urgent nephrology review and consideration of dialysis. ✔️ Treat the cause, not just the creatinine. 📖 Want more concise, exam-focused nephrology notes? Visit mediconotes.com and explore our Nephrology & Urology book—designed for medical students, MRCP, USMLE, PLAB, AMC, and everyday clinical practice. ❤️ Save this post for revision. 📤 Share it with your colleagues. 💬 What investigation do you always order first when assessing AKI? #AKI #AcuteKidneyInjury #Nephrology #InternalMedicine #MedicalStudent

💧 7 Causes of Hyponatremia Low sodium is a finding—not the diagnosis. The key is identifying the underlying mechanism. Hyponatremia (serum Na⁺ <135 mmol/L) is one of the most common electrolyte disorders encountered in clinical practice. A systematic approach using serum osmolality, volume status, and urine studies helps narrow the differential diagnosis. 📚 7 High-Yield Causes: 1️⃣ Primary Polydipsia (Excess Water Intake) • Excess free water overwhelms renal excretion. • Low urine osmolality and dilute urine. 2️⃣ SIADH • Excess ADH → water retention without oedema. • Euvolemic hyponatremia with high urine osmolality and high urine sodium. 3️⃣ Thiazide Diuretics • Common drug-induced cause, especially in elderly patients. • Causes renal sodium loss with impaired urinary dilution. 4️⃣ Hypovolemic Hyponatremia • Sodium loss exceeds water loss. • Seen with vomiting, diarrhoea, adrenal insufficiency, or diuretics. 5️⃣ Hypervolemic Hyponatremia • Total body water and sodium increase, but water retention predominates. • Common in heart failure, cirrhosis, nephrotic syndrome, and advanced CKD. 6️⃣ Adrenal Insufficiency • Cortisol deficiency increases ADH secretion. • Think of hyponatremia with hypotension, hyperkalaemia, weight loss, or hypoglycaemia. 7️⃣ Hypothyroidism • Reduced cardiac output and GFR impair free water clearance. • Usually causes mild chronic hyponatremia. 💡 Exam Pearls ✔️ Always classify hyponatremia as hypovolemic, euvolemic, or hypervolemic. ✔️ Exclude adrenal insufficiency and hypothyroidism before diagnosing SIADH. ✔️ Severe symptomatic hyponatremia requires 3% hypertonic saline. ✔️ Chronic hyponatremia must be corrected slowly to prevent osmotic demyelination syndrome (ODS). 📖 Want more concise, exam-focused notes like this? Visit mediconotes.com and explore our high-yield Nephrology & Urology book, designed for medical students, MRCP, USMLE, PLAB, AMC, and clinical practice. ❤️ Save this post for revision. 📤 Share it with your colleagues. 💬 Which cause of hyponatremia do you find hardest to remember? #Hyponatremia #Nephrology #InternalMedicine #Electrolytes #MedicalStudent

🚨 DIABETIC KETOACIDOSIS (DKA) “I’m so thirsty… and I can’t stop vomiting.” Diabetic ketoacidosis (DKA) is a life-threatening complication of diabetes caused by absolute or relative insulin deficiency, resulting in hyperglycaemia, ketosis, and metabolic acidosis. Early recognition and prompt treatment save lives. 🔑 Classic Clinical Features 1️⃣ Polyuria and polydipsia 2️⃣ Nausea, vomiting, and abdominal pain 3️⃣ Dehydration and tachycardia 4️⃣ Kussmaul breathing (deep, rapid respirations) 5️⃣ Fruity (acetone) breath 6️⃣ Altered mental status or reduced consciousness 🚨 Common Triggers • Missed insulin doses • Infection (most common) • New-onset Type 1 diabetes • Myocardial infarction • Stroke • Pancreatitis • Surgery or severe illness 🩺 Diagnosis Think DKA when you find: ✅ Blood glucose >11 mmol/L (or known diabetes) ✅ Blood ketones ≥3.0 mmol/L (or significant ketonuria) ✅ Metabolic acidosis: • pH <7.3 • Bicarbonate <15 mmol/L 💉 Emergency Management 1️⃣ Start 0.9% IV saline immediately. 2️⃣ Begin a fixed-rate IV insulin infusion. 3️⃣ Monitor and replace potassium carefully. 4️⃣ Identify and treat the underlying trigger. 5️⃣ Monitor glucose, ketones, electrolytes, venous blood gas, urine output, and vital signs regularly. ⚠️ High-Yield Pearl Never stop long-acting (basal) insulin during DKA treatment unless specifically advised. Watch closely for: 🚨 Cerebral oedema 🚨 Hypokalaemia 🚨 Acute kidney injury 🚨 Hypoglycaemia during treatment 💡 Remember DKA = Dehydration + Ketosis + Metabolic Acidosis Early fluids, insulin, electrolyte replacement, and treatment of the precipitating cause are the cornerstones of management. 📚 Save this post and visit our website for innovative high-yield medical notes: MedicoNotes.com #DKA #DiabeticKetoacidosis #Diabetes #Endocrinology #EmergencyMedicine #AcuteMedicine #CriticalCare #MedEd #MedicalEducation #FOAMed #MedicalStudents #Doctors #MRCP #USMLE #PLAB #MedicoNotes
⚠️ ANAPHYLAXIS “My throat feels like it’s closing…” Anaphylaxis is a life-threatening, rapidly progressive systemic allergic reaction that requires immediate recognition and treatment. Delayed treatment can result in airway obstruction, cardiovascular collapse, and death. 🚨 Common Triggers • Foods (nuts, shellfish, milk, eggs) • Medications (penicillins, NSAIDs) • Insect stings (bees, wasps) • Latex • Contrast media 🔑 Clinical Features 1️⃣ Airway Throat tightness Hoarse voice Tongue or lip swelling Stridor 2️⃣ Breathing Shortness of breath Wheeze Hypoxia Tachypnoea 3️⃣ Circulation Hypotension Tachycardia Dizziness or collapse Syncope 4️⃣ Skin & Mucosa Urticaria (hives) Generalised itching Flushing Angioedema 5️⃣ Gastrointestinal Abdominal pain Vomiting Diarrhoea 🩺 Diagnosis Anaphylaxis is a clinical diagnosis. Suspect anaphylaxis when there is: ✅ Sudden onset illness PLUS ✅ Airway and/or breathing and/or circulation compromise AND usually skin or mucosal changes (although skin signs may be absent). 💉 Emergency Management (ABCDE) 1️⃣ Call for help immediately. 2️⃣ Give IM Adrenaline into the anterolateral thigh without delay. • Adults: 500 micrograms (0.5 mL of 1:1000) • Repeat every 5 minutes if symptoms persist. 3️⃣ High-flow oxygen. 4️⃣ Lay the patient flat with legs elevated (avoid sudden standing). 5️⃣ Establish IV access and give IV fluids if hypotensive. 6️⃣ Nebulised salbutamol for persistent wheeze. 7️⃣ Antihistamines and corticosteroids are adjuncts only—they must never delay adrenaline. 💡 High-Yield Pearl Adrenaline is the first-line treatment. There are no absolute contraindications to IM adrenaline in suspected anaphylaxis. Always observe patients after recovery, identify the trigger, prescribe an adrenaline auto-injector when appropriate, and arrange specialist allergy follow-up. 📚 Save this post and visit our website for innovative high-yield medical notes: MedicoNotes.com #Anaphylaxis #EmergencyMedicine #AcuteMedicine #Allergy #Resuscitation #CriticalCare #MedEd #MedicalEducation #FOAMed #MedicalStudents #Doctors #MRCP #USMLE #PLAB #MedicoNotes
🌀 7 CAUSES OF VERTIGO Vertigo is a symptom, not a diagnosis. When a patient complains of “dizziness,” the key question is: ❓ Is this true vertigo (a false sensation of movement) or something else? Correctly distinguishing peripheral from central causes is essential, as some causes are benign, while others may represent a neurological emergency. 🔑 Common Causes of Vertigo 1️⃣ BPPV (Benign Paroxysmal Positional Vertigo) • Most common cause • Brief episodes triggered by head movement • No hearing loss • Positive Dix-Hallpike test • Treated with the Epley manoeuvre 2️⃣ Vestibular Neuritis • Acute severe vertigo lasting days • Often follows a viral illness • Nausea and vomiting common • No hearing loss 3️⃣ Ménière Disease • Recurrent episodes of vertigo • Fluctuating hearing loss • Tinnitus and aural fullness • Usually unilateral 4️⃣ Vestibular Migraine • Vertigo associated with migraine features • Photophobia, phonophobia, aura • May occur without headache 5️⃣ Labyrinthitis • Vertigo + hearing loss • Often post-viral • Auditory and vestibular symptoms occur together 6️⃣ Acoustic Neuroma (Vestibular Schwannoma) • Progressive unilateral hearing loss • Tinnitus • Gradual onset imbalance or vertigo 7️⃣ Central Causes 🚨 • Stroke • Multiple sclerosis • Cerebellar tumours • Brainstem lesions ⚠️ Red Flags Suggesting a Central Cause 🚨 Diplopia 🚨 Dysarthria 🚨 Limb weakness 🚨 Severe ataxia 🚨 New headache 🚨 Persistent neurological deficits 🩺 Clinical Approach ✔️ Take a careful history ✔️ Examine for nystagmus ✔️ Perform the HINTS examination when appropriate ✔️ Assess hearing ✔️ Look for focal neurological signs 💡 High-Yield Pearl Peripheral vertigo is common, but never miss a central cause. Remember: 🧠 Acute vertigo + neurological signs = Stroke until proven otherwise. 📚 Save this post and visit our website for innovative high-yield medical notes: MedicoNotes.com #Vertigo #Neurology #BPPV #MeniereDisease #vestibularneuritis

🧠 MYASTHENIA GRAVIS “My eyelids become heavier as the day goes on.” Myasthenia Gravis (MG) is an autoimmune disorder of the neuromuscular junction characterized by fluctuating, fatigable muscle weakness that typically worsens with activity and improves with rest. 🔑 Key Clinical Features ➊ Ptosis (drooping eyelids) ➋ Diplopia (double vision) ➌ Fatigable muscle weakness ➍ Bulbar symptoms: dysarthria, dysphagia, chewing difficulty ➎ Proximal limb weakness ➏ Respiratory muscle weakness in severe cases 💡 High-Yield Pearl MG fluctuates throughout the day: ⬇️ Worse with activity ⬆️ Improves with rest Remember: 🧊 Ice pack test → transient improvement in ptosis. 🔍 Diagnosis • Anti-AChR antibodies (most common) • Anti-MuSK antibodies • Repetitive nerve stimulation • Single-fiber EMG (most sensitive) • CT/MRI chest to exclude thymoma ⚠️ Myasthenic Crisis Watch for: 🫁 Respiratory distress 🗣️ Severe bulbar weakness 🚨 Inability to count to 20 in one breath These patients require urgent assessment and may need ICU admission. 💊 Treatment • Pyridostigmine • Corticosteroids • Azathioprine/Mycophenolate • IVIG or Plasma Exchange in severe disease • Thymectomy in selected patients 📚 Save this post and visit our website for innovative high-yield medical notes: MedicoNotes.com #MyastheniaGravis #Neurology #NeuroTwitter #MedEd #medicaleducation
💡5 ENDOCRINE EMERGENCIES YOU MUST NEVER MISS! 1️⃣ DKA (Diabetic Ketoacidosis) • Hyperglycaemia + ketosis + metabolic acidosis • Common triggers: infection, missed insulin, MI, surgery • Treatment: IV fluids → insulin → potassium replacement 2️⃣ HHS (Hyperosmolar Hyperglycaemic State) • Severe hyperglycaemia (>600 mg/dL) with profound dehydration • Minimal or absent ketones • Often occurs in elderly patients with type 2 diabetes • Requires aggressive fluid resuscitation 3️⃣ Thyroid Storm • Life-threatening decompensated hyperthyroidism • Features: fever, tachyarrhythmias, delirium, diarrhoea • Remember the 4 P’s: Propranolol → PTU → Potassium iodide → Prednisolone 4️⃣ Myxedema Coma • Severe hypothyroidism presenting with hypothermia, bradycardia, hypotension, and altered mental status • Always administer IV hydrocortisone before levothyroxine 5️⃣ Adrenal Crisis • Presents with refractory hypotension, abdominal pain, vomiting, hyponatraemia, hyperkalaemia, and hypoglycaemia • Immediate treatment with IV hydrocortisone and fluids is lifesaving 💡 High-Yield Exam Pearls: ✅ DKA = ketones present | HHS = ketones absent ✅ Treat thyroid storm empirically — don’t wait for investigations ✅ Replace potassium before insulin if K⁺ < 3.3 mmol/L ✅ Always consider adrenal crisis in unexplained shock ✅ Endocrine emergencies are true medical emergencies — act fast! 📌 Save this post for revision and share it with your colleagues. 📚 Visit our website site: MedicoNotes.com Explore our comprehensive Endocrinology Book. ——————- #Endocrinology #USMLE #medicine #doctorsofinstagram #MedEd




🫁 ACUTE PULMONARY EMBOLISM (PE) Acute pulmonary embolism is a potentially life-threatening emergency caused by obstruction of the pulmonary arteries, most commonly due to thrombi arising from the deep veins of the lower limbs. Early recognition and prompt treatment can be lifesaving. - Typical Clinical Features ➊ Sudden onset dyspnoea ➋ Pleuritic chest pain ➌ Tachycardia ➍ Hypoxia/desaturation ➎ Tachypnoea ➏ Haemoptysis ➐ Syncope or presyncope ➑ Anxiety or a sense of impending doom 🚨 Important Risk Factors • Recent surgery or trauma • Prolonged immobilisation or hospitalisation • Long-distance travel • Previous DVT or PE • Active cancer • Pregnancy and puerperium • Combined oral contraceptive pill or HRT • Obesity • Thrombophilia 🔍 Examination Findings • Tachycardia • Tachypnoea • Hypoxia • Raised JVP • Signs of DVT (unilateral leg swelling, calf tenderness) • Hypotension in massive PE 🩺 Diagnostic Approach 1️⃣ Assess clinical probability using Wells or Geneva score. 2️⃣ Low/intermediate probability: → D-dimer testing. 3️⃣ High probability or positive D-dimer: → CT Pulmonary Angiography (CTPA) is the investigation of choice. 4️⃣ If haemodynamically unstable: → Urgent bedside echocardiography and immediate senior review. 💡 ECG Findings (High Yield) • Sinus tachycardia (most common) • S1Q3T3 pattern • Right bundle branch block • T-wave inversion in V1–V4 • Right axis deviation 💡 High-Yield Pearl Think PE in any patient presenting with: 🫁 Sudden breathlessness ❤️ Pleuritic chest pain ⚡ Tachycardia 🩸 Risk factors for venous thromboembolism Remember: 🩸 DVT + Dyspnoea = Exclude PE until proven otherwise. ⚠️ Massive PE presenting with shock or hypotension is a medical emergency and may require thrombolysis, catheter-directed therapy, or surgical embolectomy. 📚 Save this post and visit our website for innovative high-yield medical notes: MedicoNotes.com #PulmonaryEmbolism #PE #RespiratoryMedicine #EmergencyMedicine #InternalMedicine
💡Cushing’s Syndrome Cushing’s syndrome results from prolonged exposure to excess cortisol and presents with a characteristic constellation of clinical features. Recognizing these features early is essential for diagnosis and management. 🔑 Classic features include: ✅ Central obesity ✅ Moon facies ✅ Buffalo hump ✅ Purple abdominal striae ✅ Proximal muscle weakness ✅ Hypertension ✅ Hyperglycaemia/diabetes ✅ Easy bruising and thin skin ✅ Osteoporosis ✅ Mood changes and depression 🩺 Common causes: • Prolonged corticosteroid use (most common) • Pituitary adenoma (Cushing disease) • Adrenal adenoma/carcinoma • Ectopic ACTH production (e.g., small cell lung cancer) 💡 High-Yield Pearl: Think Cushing’s syndrome in patients with central obesity, proximal myopathy, hypertension, and purple striae. Save this post for revision and share it with your colleagues! 📚 Looking for comprehensive, exam-focused Endocrinology notes? 📖 Visit MedicoNotes.com and explore our high-yield Endocrinology Book—designed to help medical students and doctors master endocrinology with ease. #CushingsSyndrome #Endocrinology #MedicalEducation #MedStudent #medicalschool
🩺 Nephrotic Syndrome: The 4 Classic Features You Must Know! Nephrotic syndrome is a common and high-yield nephrology topic that every medical student and healthcare professional should recognize. The diagnosis is based on four key features—remember them, and you’ll never miss the diagnosis! 🔍 Here are the 4 classic criteria of nephrotic syndrome: 1️⃣ Heavy Proteinuria 🧪 Urinary protein loss >3.5 g/day 💡 Massive protein loss is the hallmark of nephrotic syndrome. 2️⃣ Hypoalbuminaemia 🩸 Low serum albumin (<30 g/L) 💡 Loss of albumin in the urine reduces plasma oncotic pressure. 3️⃣ Hyperlipidaemia 📈 Elevated cholesterol and triglycerides 💡 The liver increases lipoprotein production in response to low albumin levels. 4️⃣ Generalised Oedema 🦵 Peripheral oedema, facial puffiness, or anasarca 💡 Reduced oncotic pressure leads to fluid accumulation in tissues. 🔎 Common causes include: • Minimal Change Disease • Focal Segmental Glomerulosclerosis (FSGS) • Membranous Nephropathy • Diabetic Nephropathy • Amyloidosis • Lupus Nephritis 💊 Management principles: ✔️ Treat the underlying cause ✔️ Salt restriction and diuretics ✔️ ACE inhibitors/ARBs to reduce proteinuria ✔️ Manage hyperlipidaemia ✔️ Monitor for complications such as thrombosis and infection ————— 📚 Visit our website to download our new nephrology book: mediconotes.com ———— #Nephrology #NephroticSyndrome #MedicalSchool #MRCP #usmle
🧠 8 Adult Brain Tumor Buzzwords You MUST Know! Brain tumors are among the highest-yield topics in neurology, radiology, pathology, and the USMLE. Recognizing classic presentations and pathology buzzwords can help you diagnose the lesion before seeing the answer choices! 🔍 Here are 8 essential adult brain tumors every medical student should know: 1️⃣ Glioblastoma (GBM) 🦋 Butterfly lesion crossing the corpus callosum 🔬 Pseudopalisading necrosis 💡 Most common malignant primary brain tumor in adults 2️⃣ Meningioma 📍 Extra-axial, dural-based tumor with a dural tail 🔬 Whorled cells + psammoma bodies 💡 Common in middle-aged women 3️⃣ Oligodendroglioma 🍳 Fried egg cells + chicken-wire capillaries 📍 Usually arises in the frontal lobe 💡 Think calcified frontal lobe tumor 4️⃣ Vestibular Schwannoma 👂 Unilateral hearing loss + tinnitus + vertigo 📍 Cerebellopontine angle (CPA) mass 💡 Bilateral lesions suggest NF2 5️⃣ Pituitary Adenoma 👁️ Bitemporal hemianopia from optic chiasm compression 🍼 Prolactinoma → galactorrhea and amenorrhea 💡 Cabergoline is first-line for prolactinomas 6️⃣ Primary CNS Lymphoma 🦠 Associated with immunosuppression and EBV 📍 Periventricular enhancing lesions 💡 Consider in HIV/AIDS patients 7️⃣ Hemangioblastoma 🩸 Cerebellar cystic lesion with mural nodule 📈 Increased erythropoietin → polycythemia 💡 Associated with Von Hippel-Lindau syndrome 8️⃣ Brain Metastases 🎯 Multiple lesions at the gray-white junction 📍 Common primaries: lung, breast, melanoma, kidney, and colon 💡 Metastases are the most common brain tumors in adults 📚 Save this post for revision and share it with your study partner! For more high-yield Neurology notes, mnemonics, and exam-focused summaries, visit MedicoNotes.com #Neurology #BrainTumors #USMLE #MedicalSchool #MedStudent #NeurologyNotes #Radiology #Pathology #FOAMed #MedEd #MedicalEducation #Neurosurgery #USMLEStep1 #USMLEStep2 #PLAB #MRCP #MedicalStudents #MedicoNotes #BrainTumor #Neuroanatomy


🧠 8 Movement Disorder Localizations Movement disorders can arise from lesions at multiple levels of the nervous system. Recognizing the clinical pattern is key to accurate localization and diagnosis. 1️⃣ Basal Ganglia 🔹 Disorders: Parkinsonism, chorea, dystonia 🔹 Clues: Resting tremor, rigidity, bradykinesia, abnormal postures 🔹 Common causes: Parkinson’s disease, Huntington’s disease, drugs, stroke 2️⃣ Thalamus 🔹 Disorders: Tremor, hemiballismus 🔹 Clues: Contralateral involuntary movements 🔹 Common causes: Stroke, hemorrhage, multiple sclerosis 3️⃣ Cerebellum 🔹 Disorders: Ataxia, intention tremor, dysmetria 🔹 Clues: Gait instability, nystagmus, dysdiadochokinesia 🔹 Common causes: Stroke, tumors, alcohol, multiple sclerosis 4️⃣ Brainstem 🔹 Disorders: Tremor, dystonia, parkinsonism 🔹 Clues: Cranial nerve deficits with long tract signs 🔹 Common causes: Stroke, tumors, neurodegenerative diseases 5️⃣ Spinal Cord 🔹 Disorders: Spasticity, clonus, segmental myoclonus 🔹 Clues: UMN signs below the lesion with sensory level 🔹 Common causes: Trauma, transverse myelitis, multiple sclerosis 6️⃣ Motor Cortex 🔹 Disorders: Focal motor seizures, apraxia, myoclonus 🔹 Clues: Cortical signs, seizures, contralateral weakness 🔹 Common causes: Stroke, tumors, encephalitis 7️⃣ Peripheral Nerves 🔹 Disorders: Fasciculations, weakness, occasional tremor 🔹 Clues: LMN signs including atrophy and fasciculations 🔹 Common causes: Peripheral neuropathy, entrapment, motor neuron disease 8️⃣ Neuromuscular Junction / Muscle 🔹 Disorders: Fatigable weakness, myopathies 🔹 Clues: Ptosis, diplopia, proximal weakness, fatigability 🔹 Common causes: Myasthenia gravis, inflammatory myopathies, muscular dystrophies ———————— 📚 Master neurological localization with our comprehensive MedicoNotes Neurology Book—packed with high-yield diagrams, clinical pearls, and exam-focused summaries. 🌐 mediconotes.com ————————- #Neurology #MovementDisorders #ParkinsonDisease #NeurologyResident #MedicalEducation

🧠 MIGRAINE: More Than Just a Headache! Migraines affect millions worldwide and are far more than “just a bad headache.” Recognizing the symptoms and triggers can help patients seek early treatment and improve quality of life. 1️⃣ What is Migraine? ➊ A neurological disorder characterized by recurrent attacks of moderate to severe headache. ➋ Often associated with nausea, vomiting, and sensitivity to light and sound. ➌ May occur with or without aura. 2️⃣ Common Symptoms ➊ Throbbing or pulsating headache (often unilateral) ➋ Nausea and/or vomiting ➌ Photophobia (light sensitivity) ➍ Phonophobia (sound sensitivity) ➎ Visual disturbances or aura in some patients 3️⃣ Common Triggers ➊ Stress and anxiety ➋ Sleep deprivation or irregular sleep patterns ➌ Bright lights or loud noises ➍ Certain foods and caffeine changes ➎ Hormonal fluctuations and dehydration 4️⃣ Red Flag Features 🚨 Seek urgent medical attention if headache is associated with: ➊ Sudden onset “thunderclap” headache ➋ New neurological deficits or confusion ➌ Fever or meningism ➍ Head trauma ➎ Progressive worsening pattern 5️⃣ Management ➊ Avoid known triggers ➋ Maintain good hydration and regular sleep ➌ Acute treatment: NSAIDs, triptans, antiemetics ➍ Preventive therapy for frequent attacks (e.g., propranolol, topiramate, CGRP inhibitors) 💡 High-Yield Pearl: The mnemonic POUND helps identify migraine: Pulsatile • One-day duration (4–72 h) • Unilateral • Nausea/vomiting • Disabling intensity. 📚 Looking for concise, high-yield neurology revision notes? Visit mediconotes.com and explore our comprehensive Neurology Book designed for medical students and healthcare professionals. 🌐 mediconotes.com #Migraine #Neurology #Headache #MedicalEducation #MedEd
❤️ 7 ECG Emergencies Every Clinician Must Recognize Early recognition of ECG emergencies saves lives. Here are seven ECG patterns you should never miss: 1️⃣ STEMI • ST elevation in ≥2 contiguous leads • Indicates acute coronary occlusion 💡 Pearl: Activate the cath lab immediately. ⸻ 2️⃣ Hyperkalemia • Tall peaked T waves • Widened QRS, absent P waves in severe cases 💡 Pearl: Treat urgently with IV calcium and potassium-lowering therapies. ⸻ 3️⃣ Torsades de Pointes • Polymorphic VT with “twisting of the points” • Usually associated with prolonged QT 💡 Pearl: Give IV magnesium and defibrillate if unstable. ⸻ 4️⃣ Complete Heart Block • AV dissociation with independent P waves and QRS complexes • Often causes symptomatic bradycardia 💡 Pearl: Temporary pacing may be required. ⸻ 5️⃣ Ventricular Tachycardia • Regular broad-complex tachycardia 💡 Pearl: Assume VT until proven otherwise. ⸻ 6️⃣ Brugada Syndrome • Coved ST elevation in V1–V3 • Associated with sudden cardiac death 💡 Pearl: Patients may require ICD implantation. ⸻ 7️⃣ Wellens Syndrome • Biphasic or deeply inverted T waves in V2–V3 • Suggests critical proximal LAD stenosis 💡 Pearl: Avoid stress testing—urgent angiography is needed. 🧠 High-Yield Takeaway: Early ECG recognition changes outcomes and saves lives. 📚 Save this post for future revision. 🌐 Visit mediconotes.com for comprehensive high-yield cardiology notes and exam resources. #Cardiology #ECG #ECGInterpretation #MedicalEducation #MedEd


Montserrat Campos @MosherrathRoo
119 Followers 2K Following Chingandole duro • Médico • colaboro en DYNAMIC TRAVEL• escribo lo que sueño • Me gustan las margaritas • Mucho más español que inglés.


edward mutuku @eddymutuku
41 Followers 307 Following
michelle @michelleyt0xs
220 Followers 1K Following
Ruby Nguyễn @_Ruby_Nguyen_
37 Followers 115 Following
@Akarshan_Kathramalla @Akarshan_Sonu
42 Followers 939 Following @AlluArjun♥️! @imvkohli👑! @Smrithimandhana💕..
Markus Sunoto @MarkusSunoto
6 Followers 135 Following
Dickson Lukeine @DLukeine
40 Followers 424 Following
Juan Tabares @JuanTabare4727
7 Followers 538 Following

ARVIND SINGH ASWAL �... @CognisantDoc
60 Followers 324 Following 🇮🇳 Rationalist | Science Enthusiast

Zia Afghan @ziasayzz
3K Followers 3K Following War victim, clinical pharmacologist, Pharmacotherapy, infectious diseases, metabolic health, AMR. PGD Global Health Diplomacy& public health.
أشرف عوده @ashrf_wdh
0 Followers 4 Following

Eltayib @EltayibIbr12158
4 Followers 96 Following
Ise-Oluwa @realDejifelix
1K Followers 2K Following Curator of ideas||Public affairs analyst||Out of the box thinker||Medic||former Fin. Sec. @ilumsailorin||former P.R.O @ilumsailorin||YNWA⚽||Oni uyì, Oni èye
pharles @pharles007
0 Followers 201 Following
aware @abdulwares12345
41 Followers 2K Following
Rajesh @Rajesh90590753
2 Followers 47 Following

ก้อนเมฆ @Cloud4Jinxiong
168 Followers 91 Following support #林锦雄 #XIONG #NEXT1DE Red note ID:CloudXBear666


Yediluz Mamani @YediluzM99659
0 Followers 44 Following
DAKONAH ALUSINE @ALUSINE8001
2 Followers 157 Following
she aF @sheaF33
0 Followers 30 Following
Neuron @Neuronmt
0 Followers 3 Following

Patrick Cheah MD @cheahwc
400 Followers 3K Following Emergency, Critical Care and Retrieval Medicine Specialist. Asia Medevac Services Medical Director. Consultant EM and Internal Med Regency Specialist Hospital
vishnu chaitanya @dr_vishnu1994
5 Followers 150 Following
Surekha @Surekha66681442
0 Followers 19 Following
Nomo Benjamin @BENN_YKLEIN
0 Followers 9 Following
Huỳnh Lan Chi @lanchi2106
0 Followers 16 Following
Rich_Makay⏺ @RoyMaka70119427
48 Followers 265 Following #Promoter, #Believer, #GreatestFun of NewArtist. #EverythingGoodisYou.#Gladihelped.#1LORD🙏 #what_Your_name_newArtist.
AhSanpo @AhSanpol5w
176 Followers 466 Following
Eugene Duncan @EugeneDunc79635
2 Followers 34 Following
Leila Inez @LeilaInez20034
0 Followers 1 Following
Tanveer Ahmad Sheikh @sheikhtan90
8 Followers 127 Following Registered Pharmacist (Bachelor of Pharmacy) JNTU,Hyderabad
andreas @andreashcxb
0 Followers 3 Following
Khaled @Khaled561812320
4 Followers 265 Following
Zeke, MD @zekelodeon
2 Followers 30 Following
Julius @Ekajulli
15 Followers 472 Following
[email protected] @muhwezi4031
4 Followers 38 Following
M @m_ip11ah
3 Followers 141 Following
Journal of Brown Hosp... @BrownJHM
325K Followers 576 Following Official account of ‘The Brown Journal’. We aim to provide practical information relevant to hospital & internal medicine. Posts ≠ medical advice.
Mushood Ahmed @MushoodCh
182 Followers 671 Following MBBS | Clinical Researcher | Cardiology & Metabolism | https://t.co/lVunBnGyZ2
Dr. Medica🩺 @DrMedica_13
46K Followers 3K Following Don’t trust the heart, it wants your blood 🩸 Doctor 👨⚕️ Social Media Activist
CORE IM @COREIMpodcast
51K Followers 5K Following Medicine Podcast || Inspiring curiosity & critical thinking || 5 Pearls || Mind the Gap || Hoofbeats || At the Bedside || Gray Matters || Biweekly Wed.

USMLE @TheUSMLE
46K Followers 265 Following The USMLE® is a three-step examination for medical licensure in the United States and is sponsored by FSMB and NBME.You might like